From Validation to Adaptation: Fine-Tuning the ECG-FM for Single-Lead Deployment
This week marked our transition from diagnosing limitations to actively adapting our models for deployment. With last week’s findings confirming that naive channel duplication is insufficient, the team shifted focus toward fine-tuning the ECG foundation model directly on duplicated single-lead inputs and tightening the end-to-end inference pipeline for real-world use.
Rather than treating the foundation model as a fixed black box, we began re-shaping it to better reflect the statistical properties and constraints of wearable ECG data. This week was less about proving what doesn’t work—and more about building what will.
Key Accomplishments This Week
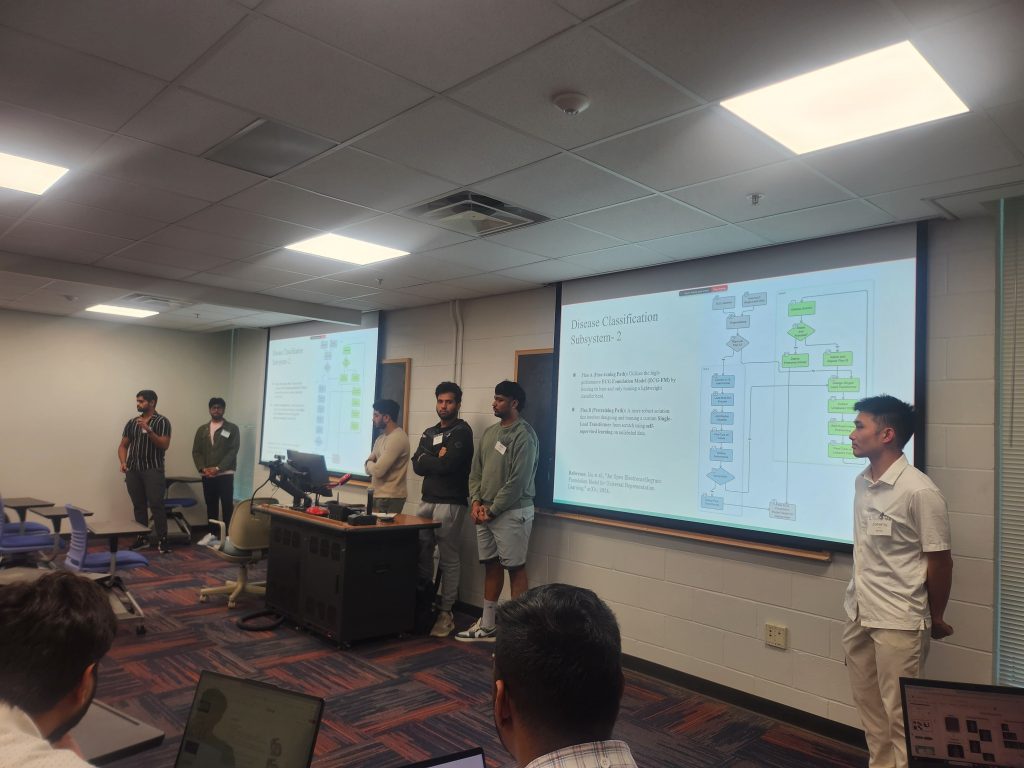
Initiated Fine-Tuning on Duplicated Single-Lead Inputs
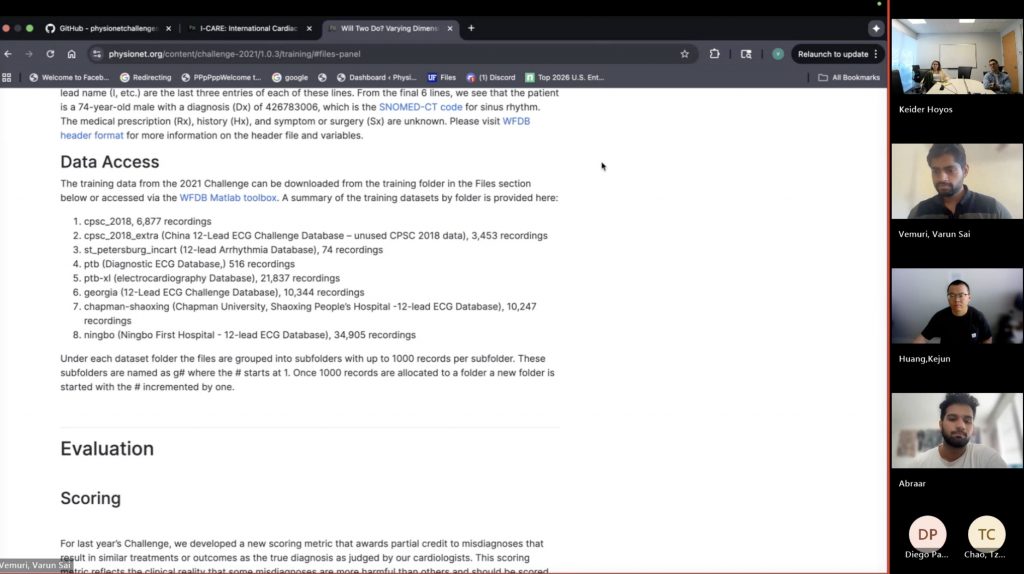
We set up the fine-tuning pipeline starting from a pretrained ECG-FM checkpoint that had not yet been biased by 12-lead-specific downstream tasks. Single-lead ECG signals were duplicated across channels to match the model’s expected input format, and supervised fine-tuning was launched for multi-label arrhythmia classification. Early training curves indicate improved stability compared to directly using the frozen multi-lead model, suggesting the model is beginning to adapt to the single-lead distribution shift.
End-to-End Inference Pipeline Prototyping
We implemented a standardized Python-based inference wrapper that takes a 5-second single-lead ECG segment as input and returns calibrated probabilities across all 17 diagnostic classes. This wrapper formalizes preprocessing, normalization, segmentation, and post-processing steps into a single callable interface, laying the groundwork for future cloud and mobile deployment.
PQRST Delineation Integration Progress
We continued refining the PQRST delineation pipeline and began aligning its input/output schema with the classification module. This included unifying windowing strategies, timestamp conventions, and output formats for fiducial points, which is critical for downstream clinical interpretation and UI integration. Initial tests confirm that both pipelines can now operate on consistent 5-second windows without manual intervention.
Calibration and Post-Processing Strategy Design
Building on last week’s observation of rare clinically implausible label combinations, we began drafting rule-based constraints and threshold calibration strategies to reduce invalid multi-label outputs. This included early experiments with probability threshold tuning and label co-occurrence filtering to improve clinical plausibility without over-constraining the model.
Sponsor Checkpoint and Deployment Alignment
We shared our fine-tuning plan and early pipeline design with Aventusoft mentors. Sponsor feedback reinforced the importance of treating the inference interface as a “product surface,” not just a research artifact—emphasizing clear contracts for inputs, outputs, latency expectations, and failure modes. This helped anchor our development priorities around deployability rather than pure model performance.
Next Steps: Toward a Deployment-Ready System
In the coming week, we will:
- Continue fine-tuning the ECG-FM on duplicated single-lead data and conduct controlled comparisons against frozen baselines.
- Run more systematic evaluations on sponsor-provided ECG samples to assess real-world generalization.
- Finalize the unified inference API for both classification and PQRST delineation, including standardized JSON-style outputs.
- Begin profiling latency and memory usage to inform future model compression and mobile deployment planning.
With the core assumptions now validated and the adaptation pipeline in motion, the project is moving from experimental prototyping toward a cohesive, deployment-oriented system. The foundation is set—now it’s about refining and hardening the stack.
See you next week!